Tracking the psychological and social waves of the pandemic: the COVID-19 Social Study
When the COVID-19 pandemic first reached the UK in early 2020, the immediate focus was on the importance of testing and tracking the development of the virus to provide regular data to policy makers and members of the public. However, it became increasingly clear that the focus of the testing and tracking was exclusively on the direct impact of the virus itself: cases and deaths. Yet it was already apparent in these early stages that the true impact of the pandemic was going to be much wider, encompassing psychological and social impacts across life domains including mental health, wellbeing, health and social behaviours, employment and education, finances, family and bereavement, access to health services, social inequalities, fears and beliefs about the pandemic, trust in institutions, and ultimately adherence to guidelines to prevent the spread of the pandemic. In other words, these broad psychological and social effects were not just secondary consequences but would ultimately determine those core metrics of cases and deaths.
Social and behavioural scientists and clinicians around the UK mobilised fast to prepare to research these psychological and social effects. In particular, researchers running the UK’s population cohort studies (such as the British Birth Cohort studies and the UK Household Longitudinal Study) started planning to run new sweeps of data collection. These cohort studies are a phenomenal resource within social and medical sciences. Their strengths include tracking individuals over time, extending back across many years to allow direct comparisons to see if factors such as mental health worsened during the pandemic; in many cases they are based on representative population samples that allow researchers to assess the prevalence of problems such as mental illness. However, a challenge with these population cohort studies is that gathering new sweeps of data takes time, and the frequency of approaches to participants has to be limited to reduce study fatigue and maintain involvement across decades of data collection. So it was clear that these studies would not be able to provide the social science research equivalent of the daily updates on cases and deaths. Further, whilst we can learn from these cohort studies how factors such as mental health differed during 2020 compared to, say, 2019, we wouldn’t necessarily know the timescale: whether mental health steadily changed over time or changed in response to specific events such as lockdown coming in.
Recognition of these research gaps inspired me and my colleagues at UCL to start the COVID-19 Social Study. Our plan was that this study would provide this crucial daily tracking on the psychological and social impact of the pandemic that could be made available to policy makers, organisations across the UK, and members of the public and allow us to understand trajectories of experiences across the pandemic. To achieve this, we designed the study around weekly follow-ups of study participants, but with participants staggered as to which day of the week they took part, to provide continuous data from each day statistically weighted to population proportions. To allow us to move fast, we could not recruit a representative sample. However, following several years’ experience in running large Citizen Science experiments plus with the support of organisations in our national UKRI MARCH Mental Health Research Network (which has over 1,400 members), we were confident we could recruit a large and diverse sample. With a focus on individual patterns and trajectories over time, our data could then be triangulated with data from the population cohort studies to understand both how much things had changed and when these changes had occurred. To support this triangulation, we collaborated with many of the population cohort studies and the Wellcome Trust to harmonise our measures wherever possible to support comparisons.
The UCL COVID-19 Social Study launched on 21st March 2020, just prior to the announcement of lockdown. Over the next few weeks, we recruited over 72,000 participants to the study, and carried out weekly monitoring of their experiences. There was an immediate demand for the data, so we started publishing weekly open access reports as well as providing further data analysis to Cabinet Office, multiple government departments, the ONS Covid Response Unit, Public Health England, NHS England, the World Health Organisation, various government and scientific Covid commissions and advisory groups, and third sector organisations such as the Red Cross and the Samaritans. There was also a clear appetite from the public for information. Across the first 6 months of the study, we’ve had 50,000 people visit the study website and 4,000 sign up for newsletter alerts to new content.
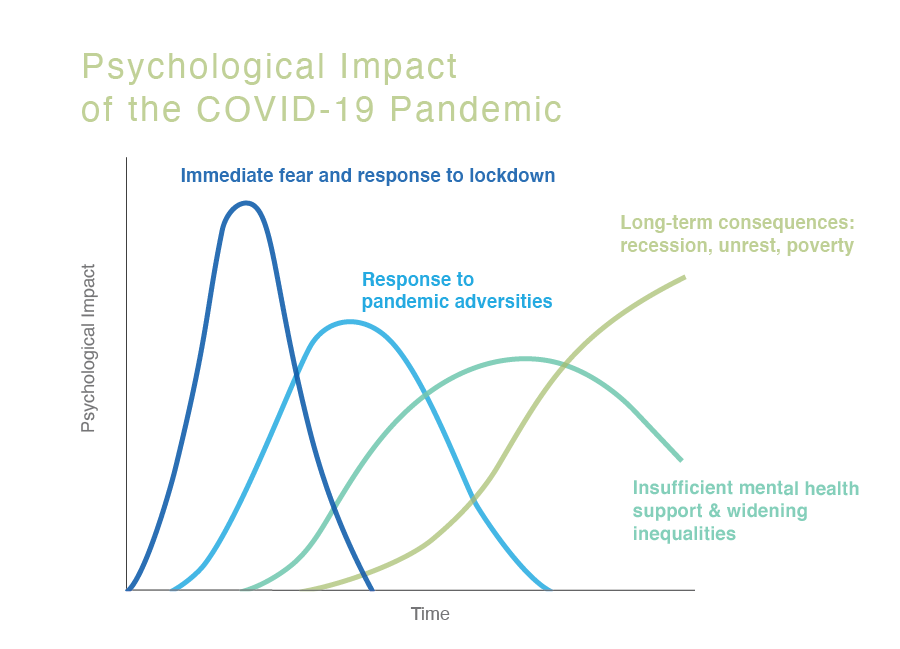
Initially, we planned the study to last for the first wave of lockdown, capturing the strict lockdown period and its easing. We had been thinking about the psychological and social impact of COVID-19 as occurring in a single wave. But during the summer of 2020 it became clear that the psychological and social impact, like the virus, would involve multiple phases, each with different types of problems. In fact, our research to date has suggested there could be at least four such phases. Whilst phase 1 has involved the immediate psychological impact of fear of the virus and the social isolation of our first lockdown, phase 2 is already underway, involving people’s response to adversities like bereavement, eviction, job losses, and financial problems as well as neurological and neuropsychiatric consequences to catching Covid-19 and experiences of ‘long Covid’. We are also predicting a third phase, with individuals not being able to access health services reliably during the pandemic, leading to potential consequences for the incidence and persistence of mental and physical health problems, as well as widening social inequalities due to ongoing adversities. Looking to the future, it’s also inevitable that there will be a fourth phase, involving the long-term impact of major consequences of the pandemic such as a recession, poverty, environmental impact, and potential social unrest.
As a result, in late August 2020, we launched a second stage of the COVID-19 Social Study. Having completed 22 weeks of weekly data collection (enabling us to track responses daily), we moved to monthly sweeps, but again staggered by week of the month for participants, enabling us to continue tracking responses across every week. Through this second stage, we plan to capture some of the second and third phases of psychological and social impact.
As for capturing that fourth phase, it remains to be seen how well we can maintain the interest of our study participants and retain their participation. Capturing such large volumes of data from so many people with such regular reassessments is already unprecedented, so we will have to ascertain whether people still have an appetite to be involved in a study for more than 12 months. However, as our approach has always been to work in tandem with the UK’s population cohort studies, this may be an opportunity for further joint work. Future sweeps of data collection on the population cohort studies will give high quality evidence as to the long-term impact of this pandemic. These data, combined with the insight gained from the COVID-19 Social Study, will allow us to understand in rich detail the ways that this pandemic has not only affected individuals as an infectious disease, but the way it is transforming our society.
Photo Credit: Jerome on Unsplash
About the author
Dr Daisy Fancourt is Associate Professor of Psychobiology & Epidemiology and Wellcome Research Fellow in the Psychobiology Group, Department of Behavioural Science & Health at UCL. Her research focuses on the effects of social factors on health, including social deficits (e.g. loneliness and social isolation) and social assets (e.g. community engagement, arts & cultural activities, and social prescribing). During the COVID-19 pandemic, Daisy has been leading the UK’s largest study into the psychological and social impact of the virus (The Covid Social Study). She also directs the COVID-Minds Network: an international network of longitudinal studies exploring the global mental health impact of the pandemic. Daisy is a member of the Lancet COVID-19 Commission and the World Health Organisation Expert Group on mental health in COVID-19.